DISCOVERY · SAFETY-CRITICAL HEALTHTECH · 2025
De-Risking Medication Management Through eMAR Discovery
Senior Product Designer (Discovery Lead) · Log my Care · July–October 2025
The Problem
When we are dealing with time critical stuff… that can be the difference to hospital admissions, life and death.
Care Manager, User Interview 6
As the product scaled, medication workflows grew more complex than the original system could support. Feature prioritisation was driven by stakeholder opinion rather than the people using it every day. No shared model of the medication lifecycle existed across the organisation.
The work focused on uncovering the root causes behind missed doses and medication errors, stock discrepancies and audit gaps, incomplete MAR charts required for CQC compliance, and workflow stress in high pressure care environments.
Every day, carers were managing high risk medications in a system that could not be consistently trusted. The cost was not just operational... It was human.

What is eMAR?
eMAR, Electronic Medication Administration Record
eMAR is the digital system care workers use to record, administer and audit medication for vulnerable adults in residential and homecare settings across the UK. It is regulated by the Care Quality Commission (CQC) and used daily by thousands of carers. Getting it wrong has direct consequences for the people in their care.
Business Context
eMAR was a commercial and safeguarding obligation, not just a product improvement.
Log my Care was expanding its homecare and residential care customer base in a competitive market. CQC inspection failures traced to medication errors carried direct commercial consequences: customer reputation, provider registration, and platform trust. A credible, CQC compliant eMAR system was a retention and acquisition lever. Providers could not seriously evaluate Log my Care without one.
Our first inspection with CQC, we got a b******ing and failed on that and it was quite frustrating.
Care Manager, Updating Medication
What I Did
I designed and ran the full research programme from scratch.
I mapped the system from the ground up, putting carer voices at the centre of every structural decision made, not internal assumptions or feature requests.
I wrote semi-structured interview guides across four focus areas: medication scheduling, PRNs and safety information, stock management, and GP/pharmacy integrations, with separate question sets for care providers and internal stakeholders.
I conducted 14 user interviews with carers, managers and support staff, synthesised in Dovetail. I ran 9 internal stakeholder sessions across Product, Engineering, Sales, Customer Success, CTO and CEO, and gathered 69 survey responses from both active and churned users. I proactively reached out to churned users myself to build participation.
In parallel I benchmarked leading eMAR competitors, ran alignment sessions with the PM, CTO and Engineering as findings emerged, and presented the full output to the whole company in in-office sessions.
What I Found
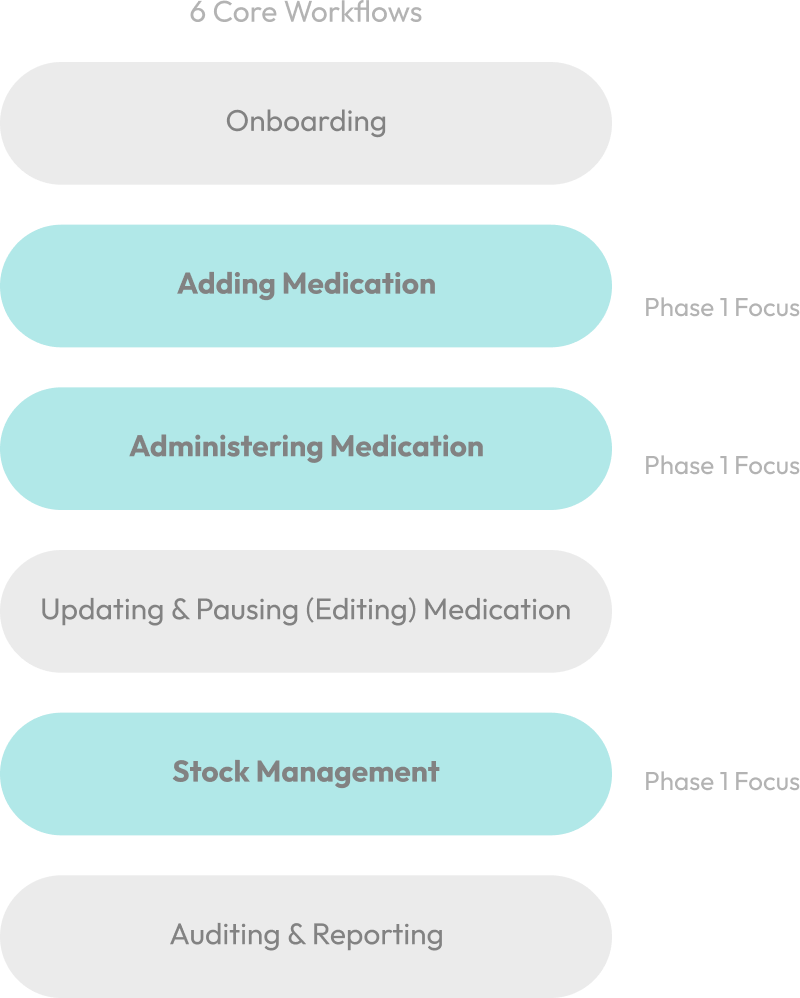
6 interdependent workflows mapped end to end for the first time.
Initial deep risk analysis focused on Adding, Administering and Stock Management due to highest frequency and safety exposure.
What emerged was not a list of UI complaints. It was a system with compounding failure modes, where a breakdown in one stage made the next stage worse, in ways no one had mapped before.
The critical insight: these were not parallel problems. They were connected, and the connections had been invisible. Unsafe editing in Adding directly created MAR accuracy gaps in Administering. Stock inconsistencies created escalation blind spots in Auditing.
What I Found
Five cross-workflow safety failure patterns from 200+ synthesised insights
These failures appeared consistently across all 14 interviews and were reflected in support tickets and usage trends.
- 01
Unsafe Medication Editing
Carers could not safely update medications without creating downstream errors.
- 02
MAR Accuracy Gaps
MAR charts were incomplete, creating CQC compliance and audit exposure.
- 03
Stock Count Inconsistency
Stock discrepancies went unresolved, creating blind spots at audit.
- 04
Escalation Visibility Gaps
No clear way to flag or escalate issues within the system.
- 05
Alert Clarity Failures
Alerts were overwhelming, unclear, or missing at the moments they mattered most.
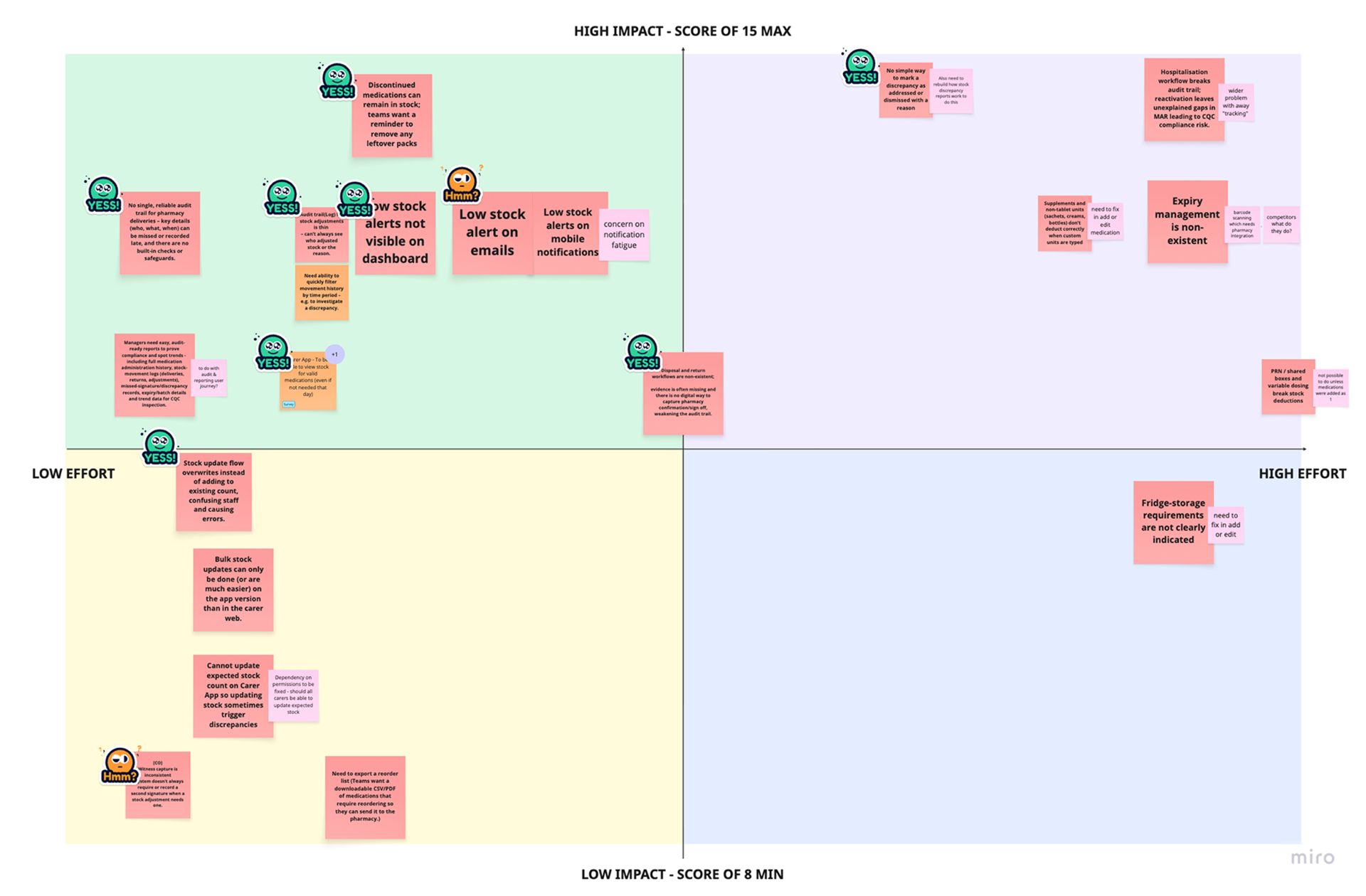
How I Prioritised
A multi-criteria model weighted toward clinical risk, not delivery speed.
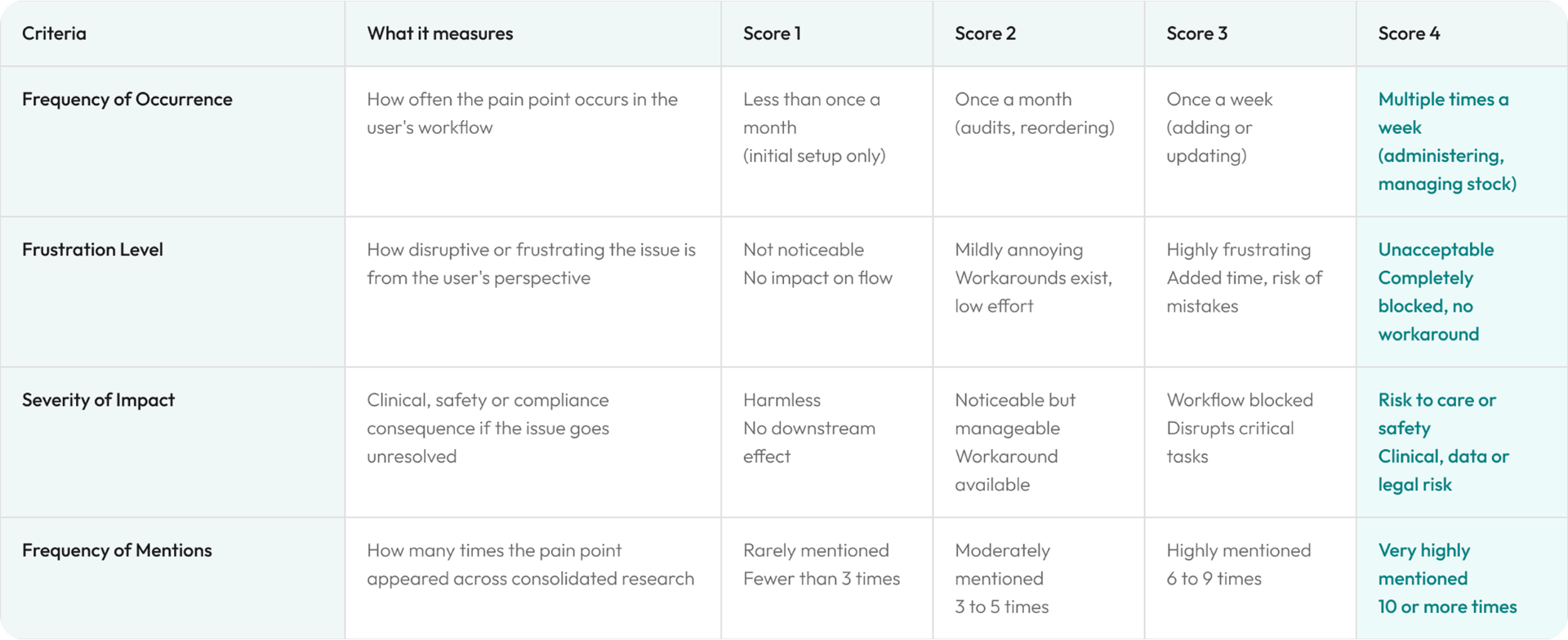
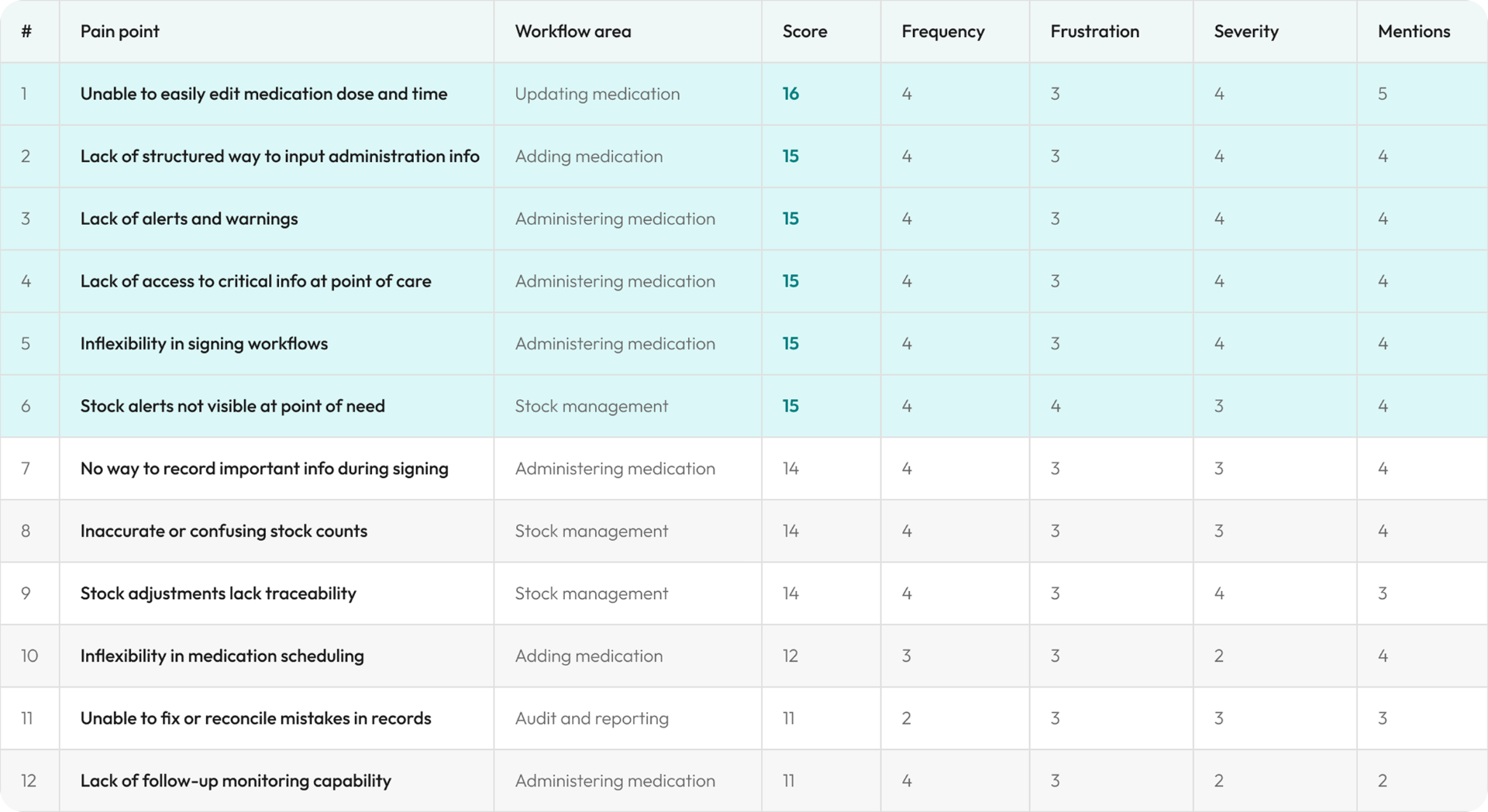
23 pain points came out of the research. A standard impact/effort matrix was not adequate. Clinical risk is not the same as user satisfaction. Something that happens rarely but puts a vulnerable person at risk outranks something causing daily friction but no harm.
I descoped two high visibility features because neither addressed any of the five structural failure patterns. Fixing the surface without addressing what was broken underneath would have created false confidence in a system that still put carers at risk. When engineering pushed to ship ahead of validation, I held the sequencing. In a CQC regulated product, shipping first and validating later is not a velocity decision. It is a safety risk.
Frequency of Occurrence
How often the pain point appears in a carer's daily workflow.
Frustration Level
How disruptive the issue is from the user's perspective.
Severity of Impact
Clinical, safety or compliance consequence if unresolved. Most heavily weighted.
Frequency of Mentions
How many times the pain point surfaced across all research sources.
Outcomes
Discovery that established the structural foundations before a screen was drawn.
The discovery did not ship a UI. It shipped the conditions for the right redesign to happen: a shared system model, a prioritised problem set, and an adopted framework that gave every team a common language.
6 workflows
mapped end to end for the first time
23
pain points scored against clinical risk
11-step
design framework adopted across five teams
Full company
findings presented to all teams in office
Churned users
proactively sourced, not just existing users
Shared model
first time the medication lifecycle was mapped org-wide
The six workflow model became the shared organisational map across Product, Engineering, Sales and Customer Success.
Problem statements, Jobs to be Done and success criteria were formally adopted by Product and Engineering.
An 11-step design solutioning framework was adopted across design, product, engineering, sales and customer success, preserving safety critical insights from discovery through to build.
What Shifted
From feature first thinking to safety first sequencing.
The discovery reframed how the organisation approached the redesign.
What I Learned
Safety critical framing lands faster when you quantify the cost of moving too fast.
Leadership wanted solutions before the system model was stable. Design rationale alone did not slow that down. I'd quantify the regulatory exposure earlier. A CQC inspection failure traced to a medication error carries a specific, tangible cost for a care provider. That number accelerates alignment faster than principled argument about methodology.
Good discovery doesn't just find problems.
It makes the people in the building feel the weight of solving them.